
Hemolytic anemia is a condition in which red blood cells are destroyed faster than the body can replace them. Normally, red blood cells live for about 120 days and carry oxygen from the lungs to tissues throughout the body. In hemolytic anemia, this lifespan becomes much shorter because the cells break down too early, leaving the body struggling to maintain enough healthy blood cells for normal function.
This can happen suddenly or gradually, and the severity varies from mild fatigue to serious complications that require urgent medical attention. Some people develop hemolytic anemia because of inherited disorders, while others experience it due to infections, autoimmune diseases, medications, or underlying medical conditions.
Understanding hemolytic anemia matters because early diagnosis often prevents complications such as severe fatigue, jaundice, gallstones, and organ stress. The good news is that many cases can be effectively managed once the cause is identified.
What Is Hemolytic Anemia?
Hemolytic anemia occurs when red blood cells are destroyed before their natural life cycle ends. This destruction process is called hemolysis. When the body detects red blood cell loss, the bone marrow tries to compensate by producing more cells. However, if destruction happens faster than production, anemia develops.
Red blood cells may break down inside blood vessels, known as intravascular hemolysis, or in organs such as the spleen and liver, called extravascular hemolysis.
Because hemoglobin is released when red blood cells break apart, the body must process this extra breakdown product. This often leads to elevated bilirubin levels, which explains why many people with hemolytic anemia develop jaundice or dark urine.
How Red Blood Cell Destruction Affects the Body
Red blood cells deliver oxygen to every organ. When too many are destroyed:
- Oxygen delivery decreases
- The heart works harder to compensate
- Fatigue becomes more noticeable
- Organs may receive less oxygen than they need
- Bilirubin builds up in the bloodstream
This explains why patients often feel weak, short of breath, dizzy, or unusually tired even after mild activity.
Causes of Hemolytic Anemia
The causes are generally divided into inherited and acquired forms.
Inherited Causes of Hemolytic Anemia
Inherited hemolytic anemia develops because of genetic abnormalities affecting red blood cells.
Sickle Cell Disease
In sickle cell disease, red blood cells become crescent-shaped instead of round. These abnormal cells break down easily and can block blood flow.
Thalassemia
Thalassemia affects hemoglobin production. Because hemoglobin is abnormal, red blood cells become fragile and are destroyed prematurely.
Hereditary Spherocytosis
This condition causes red blood cells to become sphere-shaped rather than flexible discs. These cells are quickly trapped and destroyed by the spleen.
G6PD Deficiency
Glucose-6-phosphate dehydrogenase deficiency makes red blood cells highly sensitive to oxidative stress. Certain medicines, infections, or foods can trigger sudden hemolysis.
Pyruvate Kinase Deficiency
This rare enzyme disorder weakens red blood cell energy production and shortens cell survival.
Acquired Causes of Hemolytic Anemia
Acquired hemolytic anemia develops later in life.
Autoimmune Hemolytic Anemia
The immune system mistakenly attacks healthy red blood cells.
Warm autoimmune hemolytic anemia is the most common type, while cold agglutinin disease occurs in colder temperatures.
Infections
Certain infections can directly damage red blood cells.
Examples include:
- Malaria
- Severe bacterial infections
- Viral illnesses
Medications
Some medicines may trigger immune-related hemolysis or direct red blood cell injury.
Examples include:
- Certain antibiotics
- Antimalarials
- Anti-inflammatory drugs
Blood Transfusion Reactions
If transfused blood does not match correctly, the immune system may rapidly destroy donor red blood cells.
Mechanical Destruction
Artificial heart valves and severe vascular disorders may physically damage blood cells as they circulate.
Chronic Diseases
Conditions such as lupus, lymphoma, leukemia, and kidney disorders can trigger hemolytic anemia.
Common Symptoms of Hemolytic Anemia
Symptoms vary depending on severity, speed of onset, and cause.
Fatigue and Weakness
Fatigue is often the earliest complaint because tissues receive less oxygen.
Pale Skin
A reduced red blood cell count can make the skin and inner eyelids appear pale.
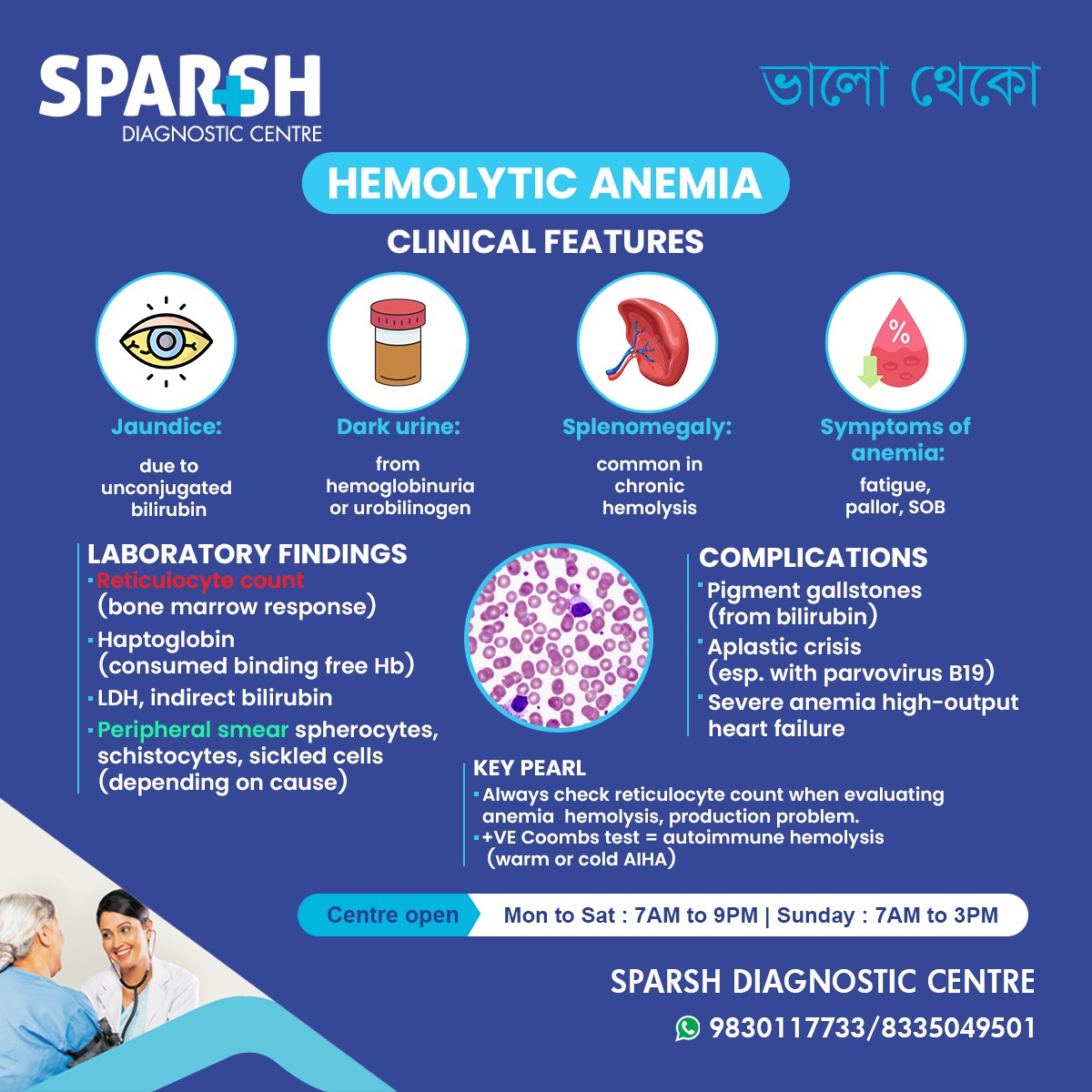
Jaundice
Yellowing of the skin and eyes happens because bilirubin rises when red blood cells break down.
Dark Urine
Hemoglobin released into the urine can create tea-colored or dark brown urine.
Shortness of Breath
Even mild activity may cause breathlessness.
Rapid Heartbeat
The heart increases output to compensate for reduced oxygen transport.
Enlarged Spleen
The spleen may enlarge because it works harder to remove damaged blood cells.
Dizziness and Headaches
Reduced oxygen delivery can affect brain circulation.
Signs Seen During Clinical Examination
Doctors often look for characteristic signs such as:
- Yellowing of the eyes
- Enlarged spleen
- Pale nail beds
- Elevated heart rate
- Signs of chronic anemia
In long-standing cases, gallstones may also develop.
Laboratory Findings in Hemolytic Anemia
Blood tests play a central role in diagnosis.
Complete Blood Count (CBC)
CBC shows low hemoglobin and often elevated reticulocyte count.
Reticulocyte Count
Reticulocytes are immature red blood cells. A high count suggests the bone marrow is trying to replace lost cells.
Peripheral Blood Smear
This helps identify abnormal red blood cell shapes such as:
- Spherocytes
- Schistocytes
- Sickle cells
Lactate Dehydrogenase (LDH)
LDH rises because damaged cells release this enzyme.
Bilirubin Levels
Indirect bilirubin increases during red blood cell breakdown.
Haptoglobin
Haptoglobin becomes low because it binds free hemoglobin released during hemolysis.
Direct Coombs Test
This confirms autoimmune hemolytic anemia by detecting antibodies attached to red blood cells.
Why Reticulocyte Count Is Important
Reticulocyte count is one of the most important clues in anemia evaluation.
A high reticulocyte count usually means:
- The bone marrow is responding properly
- Hemolysis is likely occurring
- Blood loss may also be present
A low reticulocyte count despite anemia may suggest bone marrow failure rather than hemolysis.
Types of Hemolytic Anemia
Intrinsic Hemolytic Anemia
The defect lies inside the red blood cell itself.
Examples:
- Membrane disorders
- Enzyme deficiencies
- Hemoglobin disorders
Extrinsic Hemolytic Anemia
The red blood cell is normal, but outside factors destroy it.
Examples:
- Autoimmune diseases
- Infections
- Mechanical trauma
Acute vs Chronic Hemolytic Anemia
Acute Hemolysis
Sudden red blood cell destruction can become an emergency.
Symptoms may include:
- Severe weakness
- Rapid jaundice
- Dark urine
- Fast heartbeat
- Low blood pressure
Chronic Hemolysis
Chronic cases may develop slowly and remain unnoticed for years.
Patients often adapt until symptoms worsen.
Complications of Hemolytic Anemia
If untreated, hemolytic anemia may lead to serious complications.
Gallstones
Excess bilirubin contributes to pigment gallstone formation.
Enlarged Spleen
Persistent destruction overworks the spleen.
Severe Anemia
Severe oxygen shortage stresses the heart and organs.
Heart Failure
Long-term severe anemia can lead to high-output cardiac failure.
Aplastic Crisis
Certain viral infections, especially parvovirus B19, can abruptly stop red blood cell production.
Hemolytic Anemia in Children
Children with inherited hemolytic disorders may show symptoms early.
Signs include:
- Poor growth
- Fatigue
- Repeated jaundice
- Enlarged spleen
- Bone changes in chronic severe cases
Early diagnosis helps avoid long-term complications.
Hemolytic Anemia During Pregnancy
Pregnancy can complicate management because oxygen demand rises naturally.
Close monitoring becomes important to prevent:
- Maternal fatigue
- Fetal growth problems
- Severe anemia episodes
Treatment of Hemolytic Anemia
Treatment depends entirely on the cause.
Treating the Underlying Cause
If a drug triggers hemolysis, stopping the medicine often helps.
If infection is responsible, treating the infection becomes the priority.
Corticosteroids
Steroids are often the first treatment for autoimmune hemolytic anemia because they suppress immune attack.
Blood Transfusion
Severe anemia may require transfusion, especially during acute episodes.
Immunosuppressive Therapy
When steroids do not work, doctors may use stronger immune-suppressing medicines.
Splenectomy
Removing the spleen may help certain inherited or autoimmune forms because the spleen destroys many damaged cells.
Folic Acid Supplementation
The bone marrow needs folate to produce new red blood cells rapidly.
Avoiding Triggers
Patients with G6PD deficiency must avoid known triggers such as:
- Certain drugs
- Fava beans
- Severe infections
Lifestyle Tips for Living With Hemolytic Anemia
Many people manage well with regular monitoring.
Helpful habits include:
- Staying hydrated
- Eating iron only if prescribed
- Avoiding self-medication
- Keeping vaccinations updated
- Following blood test schedules
When to Seek Medical Attention Immediately
Urgent care is needed if symptoms suddenly worsen.
Warning signs include:
- Sudden dark urine
- Severe breathlessness
- Chest pain
- Rapid jaundice
- Extreme weakness
These may indicate acute hemolysis requiring immediate treatment.
Long-Term Monitoring
Patients often need regular follow-up to monitor:
- Hemoglobin levels
- Bilirubin levels
- Spleen size
- Treatment side effects
Long-term care improves outcomes significantly.
Prognosis of Hemolytic Anemia
The outlook depends on the underlying cause.
Inherited forms often require lifelong management but can remain stable.
Acquired forms may improve completely if the trigger is identified early.
With proper treatment, many patients live normal and active lives.
FAQ About Hemolytic Anemia
What is the main cause of hemolytic anemia?
The cause depends on the type. It may result from inherited disorders, autoimmune disease, infections, medications, or blood transfusion reactions.
Is hemolytic anemia serious?
It can range from mild to severe. Some cases remain stable, while others require urgent treatment.
Can hemolytic anemia be cured?
Some acquired forms can be fully reversed if the cause is removed. Inherited forms usually need long-term management rather than cure.
Why does hemolytic anemia cause jaundice?
Destroyed red blood cells release bilirubin, which accumulates and causes yellow discoloration.
What foods help in hemolytic anemia?
A balanced diet rich in folate, vitamin B12, and nutrients supporting blood production helps overall health, though treatment depends on the cause.
Is iron useful in hemolytic anemia?
Not always. Iron should only be taken if iron deficiency is confirmed.
Can hemolytic anemia come back?
Yes, especially autoimmune forms or trigger-related cases.
Is dark urine always present?
No, but it commonly appears during active hemolysis.
To consult a Doctor at Sparsh Diagnostic Centre, call our helpline numbers 9830117733/ 8335049501.
#BhaloTheko
Disclaimer:
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.
![]()


