Red blood cells quietly work around the clock, delivering oxygen to every corner of your body. They’re essential, efficient, and constantly being renewed. But when these cells start breaking down faster than they should, the body struggles to keep up. That process is called hemolysis.
While some red blood cell breakdown is completely normal, excessive or premature destruction can lead to anemia, fatigue, jaundice, and even life-threatening complications. Understanding hemolysis—why it happens, how it feels, and what can be done about it—can make a significant difference in early detection and treatment.
Let’s break it down in simple, clear terms.
What Is Hemolysis?
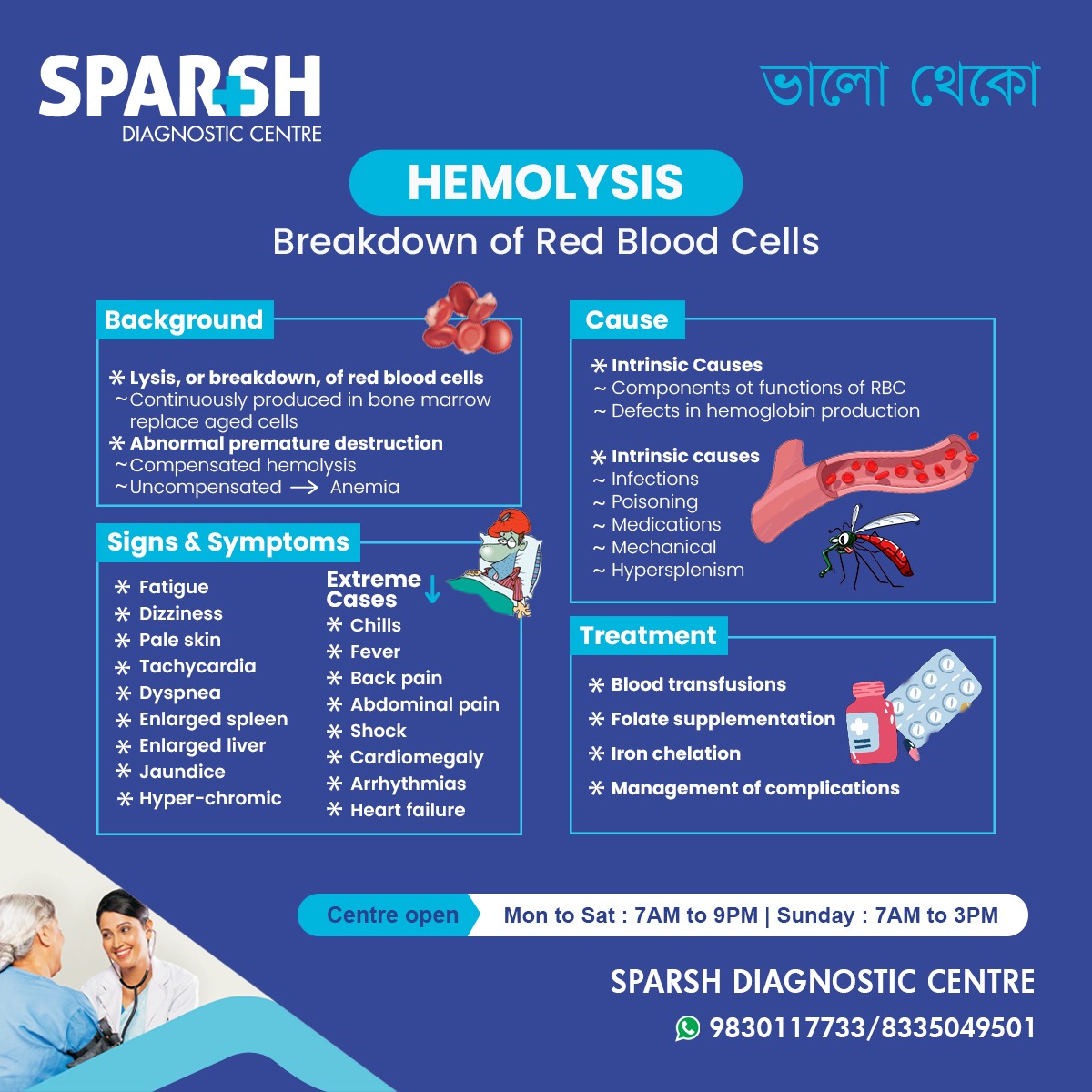
Hemolysis refers to the destruction or breakdown of red blood cells (RBCs) before their normal lifespan ends.
Under healthy conditions, red blood cells live for about 120 days. The body continuously produces new ones in the bone marrow to replace aging cells. When this balance is maintained, everything runs smoothly.
However, in hemolysis:
Red blood cells are destroyed prematurely
The bone marrow may struggle to replace them quickly enough
This imbalance can lead to hemolytic anemia
In short, hemolysis becomes a problem when destruction outpaces production.
Normal vs. Abnormal Hemolysis
Not all hemolysis is harmful.
✅ Normal (Physiological) Hemolysis
Happens naturally as red blood cells age
Old cells are removed mainly by the spleen
Bone marrow replaces them efficiently
This is part of normal body maintenance.
❌ Abnormal (Pathological) Hemolysis
Occurs when RBCs are destroyed too early
Can happen inside blood vessels (intravascular) or in organs like the spleen (extravascular)
Leads to anemia if the body cannot compensate
If the bone marrow keeps up with increased destruction, it’s called compensated hemolysis.
If it cannot, anemia develops—this is uncompensated hemolysis.
What Causes Hemolysis?
Hemolysis can occur for many reasons. Doctors typically classify causes into intrinsic (inside the red blood cell) and extrinsic (outside factors).
1. Intrinsic Causes (Problems Within the Red Blood Cell)
These are usually inherited conditions where the red blood cells themselves are abnormal.
🔹 Hemoglobin Disorders
Abnormal hemoglobin structure can make RBCs fragile.
These cells break apart more easily.
🔹 Membrane Defects
The outer structure of the RBC may be defective, causing early destruction.
Example:
Hereditary spherocytosis
🔹 Enzyme Deficiencies
Certain enzymes protect RBCs from damage.
A common example:
Without protective enzymes, cells become vulnerable to oxidative stress.
2. Extrinsic Causes (External Factors)
Here, the red blood cells are normal—but something outside them causes destruction.
🔹 Autoimmune Disorders
The immune system mistakenly attacks RBCs.
This condition is called:
Autoimmune hemolytic anemia (AIHA)
🔹 Infections
Some infections directly damage red blood cells or trigger immune reactions.
Examples:
Certain bacterial infections
🔹 Medications
Some drugs can trigger hemolysis, especially in people with enzyme deficiencies.
🔹 Mechanical Causes
Physical damage to RBCs may occur due to:
Artificial heart valves
Severe burns
Microangiopathic conditions
🔹 Toxins and Poisoning
Chemicals and snake venom can destroy RBCs rapidly.
🔹 Hypersplenism
An enlarged spleen may trap and destroy RBCs too quickly.
Symptoms of Hemolysis
Symptoms can range from mild to severe depending on how rapidly RBCs are destroyed.
Common Symptoms
Weakness
Pale skin
Because red blood cells carry oxygen, their loss often leads to classic anemia symptoms.
Severe or “Extreme” Cases
If hemolysis happens suddenly and aggressively, symptoms may escalate:
Chills
Irregular heartbeat
Acute hemolysis is a medical emergency and requires immediate attention.
Why Does Jaundice Happen in Hemolysis?
When red blood cells break down, they release hemoglobin. This eventually converts into bilirubin, a yellow pigment.
If hemolysis is excessive:
Bilirubin levels rise
The liver struggles to process it
Skin and eyes turn yellow
This is known as hemolytic jaundice.
How Is Hemolysis Diagnosed?
Diagnosis involves a combination of symptoms, medical history, and laboratory tests.
Blood Tests Doctors May Order:
Reticulocyte count (shows if bone marrow is working harder)
Lactate dehydrogenase (LDH) – elevated in hemolysis
Haptoglobin – usually low
Bilirubin levels – typically high
Peripheral blood smear
Coombs test (for autoimmune causes)
Each test provides clues about whether RBC destruction is occurring and why.
Types of Hemolysis
Understanding the type helps guide treatment.
1. Intravascular Hemolysis
Occurs inside blood vessels
Releases hemoglobin directly into circulation
May cause dark urine
2. Extravascular Hemolysis
Occurs mainly in the spleen or liver
More gradual process
Common in hereditary conditions
Treatment of Hemolysis
Treatment depends entirely on the cause and severity.
There is no one-size-fits-all approach.
1. Blood Transfusions
Used when anemia becomes severe or life-threatening.
Provides immediate relief by restoring RBC levels.
2. Treating the Underlying Cause
This may include:
Stopping an offending medication
Treating infection
Managing autoimmune disease
Addressing mechanical heart valve complications
Without treating the root cause, hemolysis will continue.
3. Corticosteroids and Immunosuppressants
Used in autoimmune hemolytic anemia to reduce immune system attack on RBCs.
4. Folate Supplementation
Hemolysis increases RBC production demand.
Folate supports new red blood cell formation.
5. Iron Chelation
In chronic cases requiring repeated transfusions, excess iron can accumulate. Chelation therapy removes excess iron from the body.
6. Splenectomy
In some hereditary or autoimmune cases, removing the spleen reduces RBC destruction.
Can Hemolysis Be Prevented?
Prevention depends on the cause.
If You Have G6PD Deficiency:
Avoid trigger medications
Avoid certain foods like fava beans
If You Have Autoimmune Conditions:
Follow treatment plans consistently
Monitor symptoms
If You Have Mechanical Heart Valves:
Regular follow-ups are essential
Genetic causes cannot be prevented—but complications can often be minimized with early detection and monitoring.
When Should You See a Doctor?
Seek medical attention if you notice:
Unexplained fatigue
Yellowing of skin or eyes
Dark brown urine
Rapid heartbeat
Persistent weakness
Sudden severe back pain
If symptoms appear suddenly or worsen rapidly, seek emergency care.
Complications of Untreated Hemolysis
Without proper treatment, hemolysis may lead to:
Severe anemia
Enlarged spleen
Heart strain
Organ damage
Shock (in acute cases)
Early diagnosis dramatically improves outcomes.
Hemolysis in Newborns
Newborn babies may experience hemolysis due to:
Blood group incompatibility (Rh or ABO)
Genetic disorders
If severe, this can cause neonatal jaundice, which may require phototherapy or exchange transfusion.
Early screening is crucial.
Living With Chronic Hemolysis
For some individuals, hemolysis is a lifelong condition.
Management typically includes:
Regular blood tests
Nutritional support
Monitoring iron levels
Avoiding triggers
Specialist care (hematologist follow-up)
With proper care, many people live healthy, productive lives.
The Bottom Line
Hemolysis isn’t just a lab finding—it’s a signal that something is disrupting your body’s oxygen delivery system.
Sometimes it’s mild and manageable. Other times, it can escalate quickly and become life-threatening.
The key is understanding:
Why it’s happening
How severe it is
What can be done about it
If caught early and treated appropriately, most cases can be controlled effectively.
Frequently Asked Questions (FAQ)
1. What is the main cause of hemolysis?
There is no single cause. It may result from inherited conditions, autoimmune diseases, infections, medications, mechanical damage, or toxins.
2. Is hemolysis the same as anemia?
No. Hemolysis refers to red blood cell destruction. If destruction exceeds production, it leads to hemolytic anemia.
3. Can hemolysis be life-threatening?
Yes, especially in acute cases where RBC destruction is rapid and severe. Immediate medical attention is necessary in such situations.
4. What are early warning signs?
Fatigue, pale skin, dark urine, jaundice, rapid heartbeat, and weakness are common early signs.
5. Can hemolysis go away on its own?
If triggered by a temporary cause (like a medication), it may resolve after removing the trigger. Chronic conditions require ongoing management.
6. How long does recovery take?
Recovery time depends on the cause and severity. Mild cases may improve in days, while chronic conditions require long-term monitoring.
7. Does hemolysis always cause jaundice?
Not always. Jaundice occurs when bilirubin levels rise significantly due to increased RBC breakdown.
8. Can stress cause hemolysis?
Stress alone does not directly cause hemolysis. However, severe infections or physical stressors may trigger it in susceptible individuals.
9. Is hemolysis contagious?
No. Hemolysis itself is not contagious. However, infections that trigger it may be.
10. Which specialist treats hemolysis?
A hematologist (blood specialist) typically manages hemolysis and related disorders.
#BhaloTheko
Disclaimer:
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.
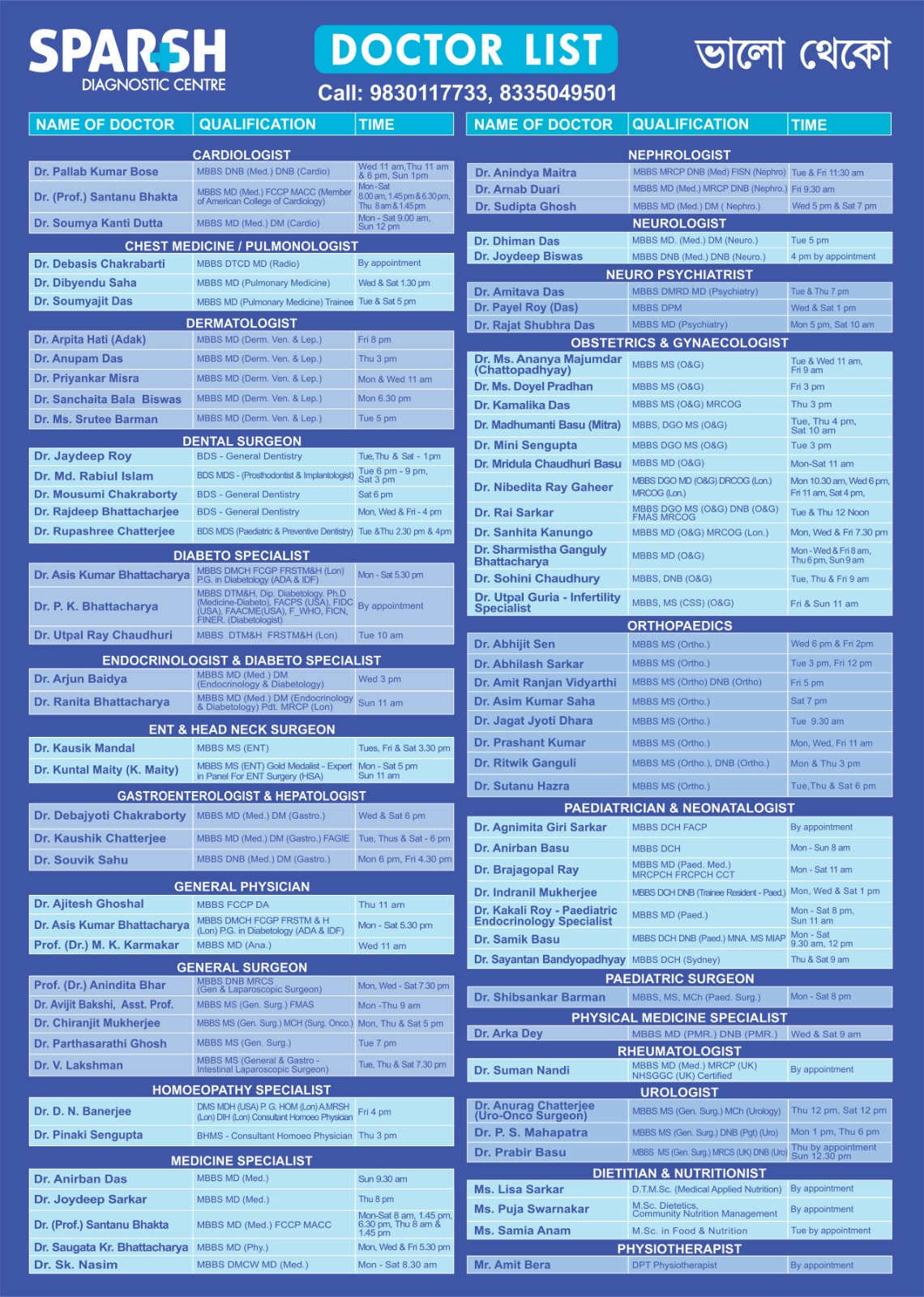
Sparsh Diagnostic Centre Doctor List
![]()