Distributive shock is a serious and potentially fatal medical emergency characterized by severe vasodilation (widening of blood vessels) that leads to inadequate blood flow to vital organs. Unlike other forms of shock where the heart fails to pump effectively or blood volume is lost, distributive shock occurs because blood vessels lose their tone and resistance, causing blood pressure to drop dramatically.
Without rapid recognition and immediate treatment, distributive shock can result in multi-organ failure and death. Understanding its causes, warning signs, and management is crucial for healthcare professionals and the general public alike.
What Is Distributive Shock?
Distributive shock is a type of circulatory shock where systemic vascular resistance decreases, causing blood to pool in peripheral vessels. This results in:
Inadequate tissue perfusion
Organ dysfunction
Despite having a normal or even increased cardiac output initially, the body cannot maintain adequate circulation due to widespread vasodilation.
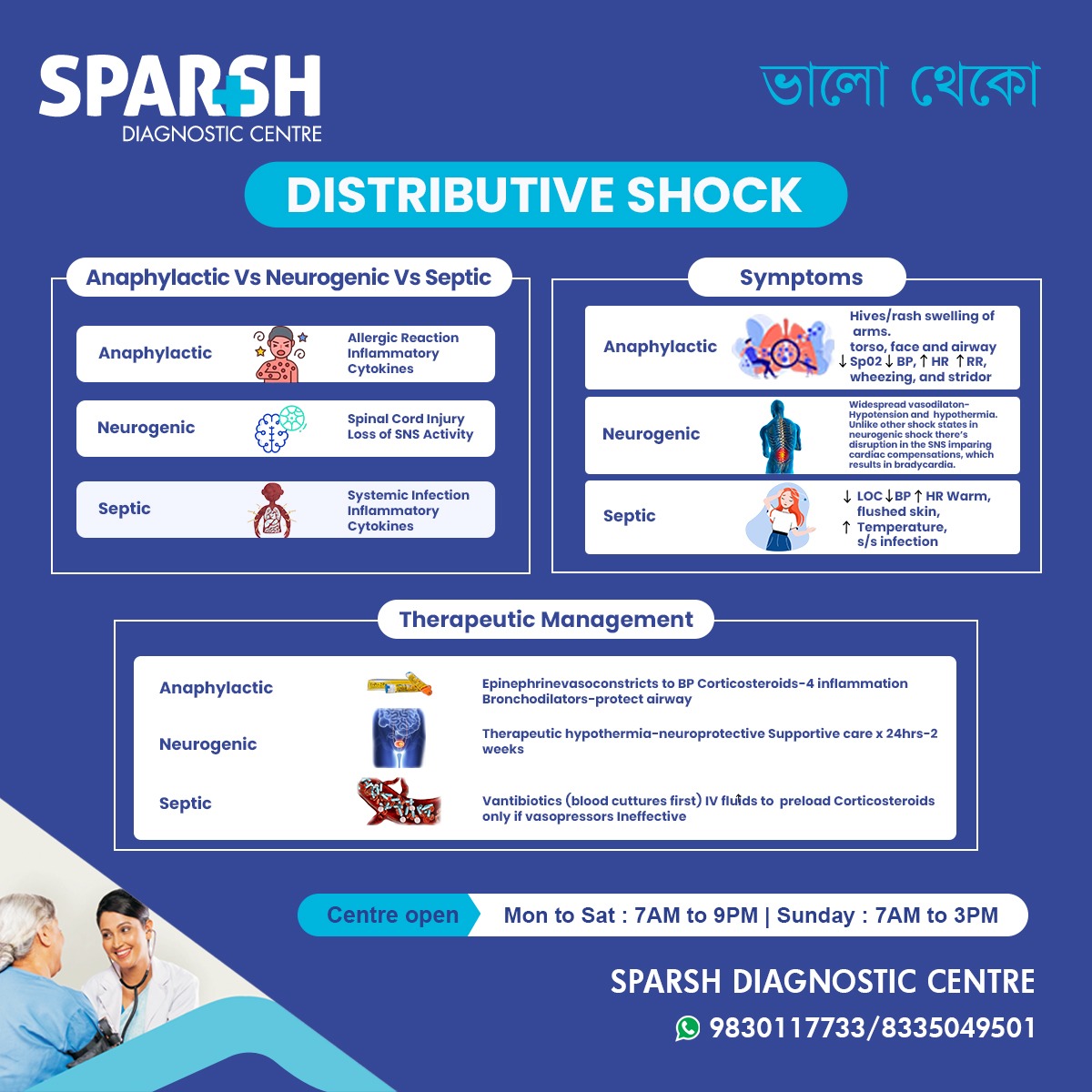
Types of Distributive Shock
It is not a single disease but a category that includes several subtypes. The three most common types are:
1. Septic Shock
Septic shock is the most common form of distributive shock. It occurs due to a severe infection that triggers a systemic inflammatory response.
Causes:
Bacterial infections (most common)
Viral infections
Fungal infections
Abdominal infections
Mechanism:
Infection triggers the release of inflammatory cytokines, leading to:
Widespread vasodilation
Increased capillary permeability
Fluid leakage into tissues
Key Symptoms:
Fever or hypothermia
Warm, flushed skin (early stage)
Altered mental status
Septic shock is associated with high mortality and requires urgent ICU management.
2. Anaphylactic Shock
Anaphylactic shock is a severe allergic reaction that causes sudden distributive shock.
Causes:
Insect stings
Medications (penicillin, NSAIDs)
Latex
Mechanism:
Allergen exposure leads to:
Massive histamine release
Rapid vasodilation
Airway swelling
Bronchospasm
Key Symptoms:
Hives and itching
Swelling of face and throat
Difficulty breathing
Sudden drop in blood pressure
Anaphylactic shock requires immediate epinephrine administration.
3. Neurogenic Shock
Neurogenic shock occurs due to injury to the spinal cord or central nervous system, leading to loss of sympathetic tone.
Causes:
Spinal cord injury (especially cervical or high thoracic)
Brain injury
Spinal anesthesia complications
Mechanism:
Damage to the sympathetic nervous system results in:
Loss of vascular tone
Severe vasodilation
Key Symptoms:
Low blood pressure
Slow heart rate (unlike other shock types)
Warm, dry skin
Loss of reflexes
Neurogenic shock differs from other shock types because it often presents with bradycardia instead of tachycardia.
Pathophysiology of Distributive Shock
To understand distributive shock, it is important to understand normal circulation.
Under normal conditions:
Blood vessels maintain tone
Blood pressure is regulated
Organs receive adequate oxygen
In distributive shock:
Blood vessels lose tone
Systemic vascular resistance drops
Blood pools in peripheral circulation
Vital organs receive insufficient oxygen
This leads to:
Cellular hypoxia
Signs and Symptoms of Distributive Shock
Although symptoms vary depending on the type, common signs include:
General Symptoms:
Low blood pressure
Rapid breathing
Altered mental status
Weak pulse
Decreased urine output
Skin Findings:
Warm, flushed skin (early septic shock)
Cold, clammy skin (late stage)
Severe Symptoms:
Loss of consciousness
Early recognition dramatically improves survival.
Causes and Risk Factors
Risk factors depend on the subtype:
Septic Shock Risk Factors:
Elderly individuals
Immunocompromised patients
Anaphylactic Shock Risk Factors:
Previous anaphylactic reaction
Neurogenic Shock Risk Factors:
Trauma
Spinal cord injury
Neurosurgical procedures
Diagnosis of Distributive Shock
Diagnosis is primarily clinical but supported by investigations.
Clinical Assessment:
Blood pressure measurement
Heart rate monitoring
Oxygen saturation
Mental status evaluation
Laboratory Tests:
Lactate levels (elevated in shock)
Arterial blood gas
Electrolytes
Imaging:
Early lactate elevation is a key marker of poor tissue perfusion.
Treatment of Distributive Shock
Distributive shock is a medical emergency requiring immediate intervention.
1. Initial Resuscitation
Airway and Breathing:
Oxygen supplementation
Mechanical ventilation if needed
Circulation:
Intravenous fluids (crystalloids)
Rapid fluid resuscitation
2. Vasopressors
If fluids do not restore blood pressure:
Norepinephrine (first-line in septic shock)
Epinephrine (especially in anaphylaxis)
Vasopressin (adjunct therapy)
Vasopressors constrict blood vessels and improve blood pressure.
3. Specific Treatments Based on Type
Septic Shock:
Broad-spectrum IV antibiotics (within 1 hour)
Source control (drain abscess, remove infected device)
Corticosteroids if refractory
Anaphylactic Shock:
Intramuscular epinephrine immediately
Antihistamines
Corticosteroids
Bronchodilators
Neurogenic Shock:
Fluid resuscitation
Vasopressors
Atropine for bradycardia
Spinal stabilization
Complications of Distributive Shock
If untreated, distributive shock can cause:
Acute kidney injury
Respiratory failure
Disseminated intravascular coagulation (DIC)
Multi-organ dysfunction syndrome (MODS)
Death
Mortality rates are highest in septic shock.
Prognosis
Prognosis depends on:
Speed of treatment
Underlying cause
Patient age
Comorbid conditions
Septic shock mortality can range from 25–50%. Anaphylactic shock has a better prognosis if treated immediately.
Early recognition is the most important predictor of survival.
Prevention Strategies
For Septic Shock:
Early treatment of infections
Vaccinations
Proper wound care
Hospital infection control
For Anaphylaxis:
Avoid known allergens
Carry epinephrine auto-injector
Wear medical alert identification
For Neurogenic Shock:
Protective gear to prevent spinal injuries
Safe driving practices
Difference Between Distributive Shock and Other Types of Shock
| Type | Cause | Cardiac Output | Skin |
|---|---|---|---|
| Hypovolemic | Blood loss | Low | Cold |
| Cardiogenic | Heart failure | Low | Cold |
| Obstructive | Blockage | Low | Cold |
| Distributive | Vasodilation | Normal/High (early) | Warm |
Distributive shock is unique because the problem lies in vascular tone, not volume or pump failure.
When to Seek Emergency Care
Seek immediate medical attention if someone experiences:
Sudden difficulty breathing
Severe allergic reaction
Confusion
Very low blood pressure
Signs of infection with weakness or fainting
Distributive shock progresses rapidly.
Frequently Asked Questions (FAQs)
1. What is the most common cause of distributive shock?
Septic shock due to severe infection is the most common cause worldwide.
2. Is distributive shock reversible?
Yes, if treated early and aggressively. Delayed treatment can lead to irreversible organ damage.
3. Why is skin warm in early distributive shock?
Vasodilation increases blood flow to the skin, making it feel warm and flushed.
4. How is septic shock different from regular sepsis?
Septic shock is a severe form of sepsis with persistent low blood pressure despite fluid resuscitation.
5. What is the first-line treatment for anaphylactic shock?
Intramuscular epinephrine is the first and most critical treatment.
6. Can neurogenic shock cause slow heart rate?
Yes, unlike other shock types, neurogenic shock often causes bradycardia due to loss of sympathetic tone.
7. How long does recovery take?
Recovery depends on severity and underlying cause. Some patients recover within days, while others may require weeks of ICU care.
8. Is distributive shock fatal?
It can be fatal without prompt treatment. Early medical care significantly improves survival.
9. What blood test indicates shock severity?
Elevated lactate levels indicate poor tissue perfusion and severity of shock.
10. Can children develop distributive shock?
Yes, especially from severe infections or allergic reactions.
Key Takeaways
Distributive shock is caused by widespread vasodilation.
Septic shock is the most common subtype.
Early symptoms include low blood pressure and warm skin.
Immediate treatment with fluids and vasopressors is critical.
Rapid intervention saves lives.
#BhaloTheko
Disclaimer:
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.
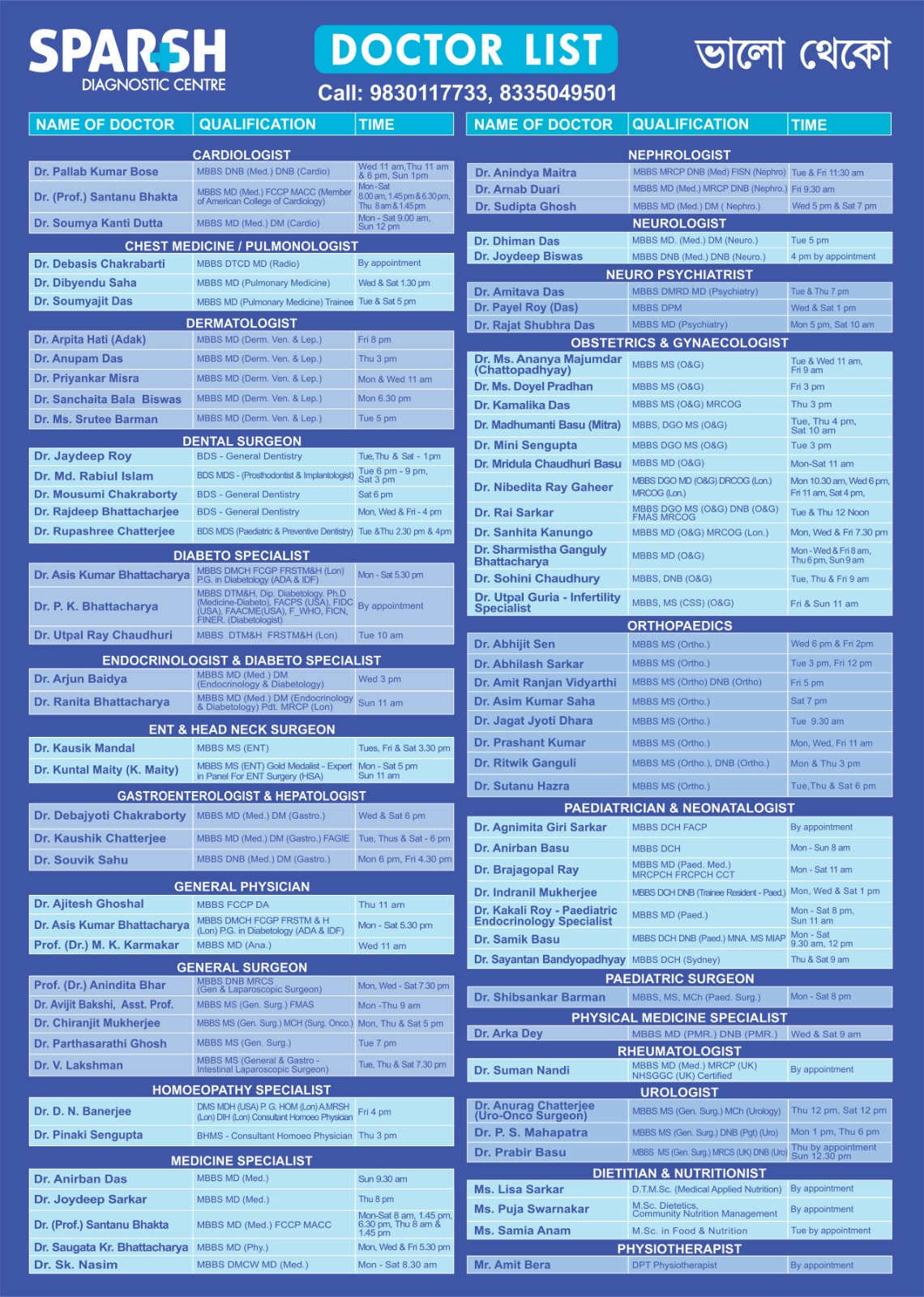
Sparsh Diagnostic Centre Doctor List
![]()