
Obesity doesn’t just affect appearance or mobility — it can deeply impact how your lungs function. One of the most serious yet under-recognized complications is Obesity Hypoventilation Syndrome (OHS).
If you or a loved one struggles with obesity and experiences constant fatigue, breathlessness, or disturbed sleep, this condition may be worth discussing with a healthcare professional. In this detailed guide, we’ll break down what OHS is, why it happens, how it’s diagnosed, and most importantly, how it can be treated effectively.
Let’s start from the basics.
What Is Obesity Hypoventilation Syndrome?
Obesity Hypoventilation Syndrome (OHS) is a breathing disorder that occurs in people with obesity. It is defined by:
Obesity (BMI ≥ 30 kg/m²)
Daytime hypercapnia (PaCO₂ > 45 mmHg) — meaning high carbon dioxide levels in the blood
No other medical cause explaining the elevated CO₂
In simple terms, the body isn’t breathing deeply or frequently enough to remove carbon dioxide properly. As a result, carbon dioxide builds up in the bloodstream, and oxygen levels may drop — a condition known as hypoxemia.
OHS is sometimes called “Pickwickian syndrome,” though that term is less commonly used in modern medicine.
Why Does Obesity Affect Breathing?
To understand OHS, it helps to understand how breathing works.
Breathing relies on:
The diaphragm
Chest wall muscles
Lung expansion
Brain signals that regulate breathing rhythm
In obesity, excess fat around the chest and abdomen restricts lung expansion. The diaphragm cannot move freely, making each breath shallower.
Over time, shallow breathing results in:
Reduced oxygen intake
Inadequate carbon dioxide removal
Chronic strain on the heart and lungs
The body’s natural drive to breathe may also become blunted in some individuals with OHS.
What Causes Obesity Hypoventilation Syndrome?
OHS doesn’t happen overnight. It develops due to a combination of factors:
1. Mechanical Restriction
Excess body fat compresses the chest wall and lungs, reducing lung capacity.
2. Impaired Respiratory Drive
Some individuals develop reduced sensitivity to carbon dioxide levels, meaning the brain doesn’t signal the body to breathe harder even when CO₂ rises.
3. Sleep-Disordered Breathing
About 90% of people with OHS also have obstructive sleep apnea (OSA). During sleep, repeated airway collapse worsens oxygen levels and increases carbon dioxide retention.
4. Hormonal and Metabolic Factors
Leptin, a hormone involved in appetite regulation, also plays a role in breathing regulation. In obesity, leptin resistance may impair respiratory stimulation.
Symptoms of Obesity Hypoventilation Syndrome
Symptoms may be subtle at first but gradually worsen. Common signs include:
Persistent daytime sleepiness
Morning headaches
Loud snoring
Poor sleep quality
Difficulty concentrating
Swelling in legs (in advanced cases)
In severe cases, patients may develop:
Many people mistake early symptoms for “just being tired” or attribute breathlessness to being overweight — which delays diagnosis.
How Is OHS Different from Obstructive Sleep Apnea?
OHS and obstructive sleep apnea often occur together, but they are not the same.
| Feature | Obstructive Sleep Apnea (OSA) | Obesity Hypoventilation Syndrome (OHS) |
|---|---|---|
| Breathing issues | During sleep only | During sleep and daytime |
| CO₂ levels | Usually normal in daytime | Elevated in daytime |
| Severity | Can vary | More serious and systemic |
In OHS, breathing remains inadequate even while awake, making it more dangerous.
How Is Obesity Hypoventilation Syndrome Diagnosed?
Diagnosis requires careful medical evaluation. Doctors typically perform:
1. Arterial Blood Gas (ABG) Test
Measures oxygen and carbon dioxide levels in the blood.
PaCO₂ > 45 mmHg confirms hypercapnia.
2. Sleep Study (Polysomnography)
Identifies sleep apnea and measures oxygen fluctuations during sleep.
3. Pulmonary Function Tests
Assess lung capacity and airflow limitation.
4. Imaging
Chest X-rays or CT scans help rule out other lung diseases.
5. Blood Tests
To exclude thyroid disorders, neuromuscular conditions, or other causes of hypoventilation.
A diagnosis is made only after ruling out other reasons for elevated carbon dioxide levels.
What Happens If OHS Is Left Untreated?
Untreated OHS can lead to serious, life-threatening complications.
1. Pulmonary Hypertension
Low oxygen levels increase pressure in lung arteries.
2. Right-Sided Heart Failure (Cor Pulmonale)
The heart struggles to pump blood against high lung pressures.
3. Respiratory Failure
Severe carbon dioxide buildup can become a medical emergency.
4. Increased Mortality
Studies show untreated OHS significantly increases the risk of death compared to obesity alone.
Early diagnosis dramatically improves outcomes.
Treatment of Obesity Hypoventilation Syndrome
The good news? OHS is treatable.
Treatment focuses on improving breathing and addressing obesity.
1. Positive Airway Pressure (PAP) Therapy
This is the cornerstone of treatment.
CPAP (Continuous Positive Airway Pressure)
Often used when OSA is present.
BiPAP (Bilevel Positive Airway Pressure)
Provides different pressures during inhalation and exhalation — especially useful for severe OHS.
These devices:
Improve oxygen levels
Reduce carbon dioxide
Improve sleep quality
Decrease strain on the heart
Many patients notice improvement within weeks.
2. Weight Loss
Weight reduction is critical.
Even a 10% weight loss can significantly improve breathing mechanics.
Options include:
Dietary changes
Structured exercise programs
Medical weight-loss therapy
Bariatric surgery (for eligible individuals)
Sustained weight loss can sometimes reverse OHS completely.
3. Oxygen Therapy
Supplemental oxygen may be added in some cases, but it is not a standalone treatment. Using oxygen alone without ventilatory support can worsen CO₂ retention.
4. Treating Associated Conditions
Managing:
Improves overall outcomes.
Lifestyle Modifications That Help
While medical therapy is essential, daily habits matter too:
Avoid alcohol and sedatives
Sleep on your side
Maintain regular sleep schedule
Follow a calorie-controlled diet
Gradually increase physical activity
Small consistent steps lead to meaningful improvements.
Who Is at Risk for OHS?
You may be at higher risk if you:
Have severe obesity (BMI > 35)
Have obstructive sleep apnea
Experience extreme daytime sleepiness
Have unexplained breathlessness
Have a large neck circumference
Men are slightly more affected, but women are not immune.
Can Obesity Hypoventilation Syndrome Be Prevented?
Prevention revolves around obesity management.
Early intervention for:
Weight gain
Snoring
Sleep apnea
Reduced exercise tolerance
Can prevent progression to OHS.
Routine health check-ups are especially important for individuals with long-standing obesity.
Prognosis: What to Expect Long-Term?
With proper treatment:
Oxygen and CO₂ levels normalize
Energy improves
Sleep becomes restorative
Risk of heart complications decreases
Without treatment, however, the condition can progressively worsen.
Adherence to PAP therapy and sustained weight loss make the biggest difference.
Frequently Asked Questions (FAQs)
1. Is Obesity Hypoventilation Syndrome life-threatening?
Yes, if untreated. It can lead to respiratory failure and heart complications. However, with early treatment, outcomes improve significantly.
2. Is OHS the same as sleep apnea?
No. While most OHS patients have sleep apnea, OHS involves elevated carbon dioxide levels even during the daytime.
3. Can weight loss cure OHS?
In many cases, significant and sustained weight loss can reverse the condition, especially if caught early.
4. Why do I get morning headaches?
Morning headaches occur due to elevated carbon dioxide levels overnight.
5. How common is OHS?
It affects approximately 10–20% of obese individuals with sleep apnea.
6. Do I need lifelong CPAP or BiPAP?
It depends. Some patients require long-term therapy, while others may reduce dependence after substantial weight loss.
7. Can children develop OHS?
It is rare but possible in adolescents with severe obesity.
8. Is oxygen alone enough?
No. Oxygen does not correct the underlying hypoventilation. Ventilatory support is usually required.
9. What BMI qualifies for OHS?
A BMI ≥ 30 kg/m² with elevated daytime CO₂ levels qualifies, though risk increases significantly above BMI 35.
10. When should I see a doctor?
Seek evaluation if you have obesity plus:
Loud snoring
Severe daytime sleepiness
Breathlessness
Morning headaches
Obesity Hypoventilation Syndrome is more than just a breathing issue — it’s a serious medical condition that reflects how excess weight can disrupt vital body functions.
The encouraging part? It’s treatable.
With early recognition, proper respiratory support, and committed weight management, patients can dramatically improve their quality of life and reduce long-term risks.
If you or someone you know experiences symptoms suggestive of OHS, don’t ignore them. A simple evaluation could make a life-saving difference.
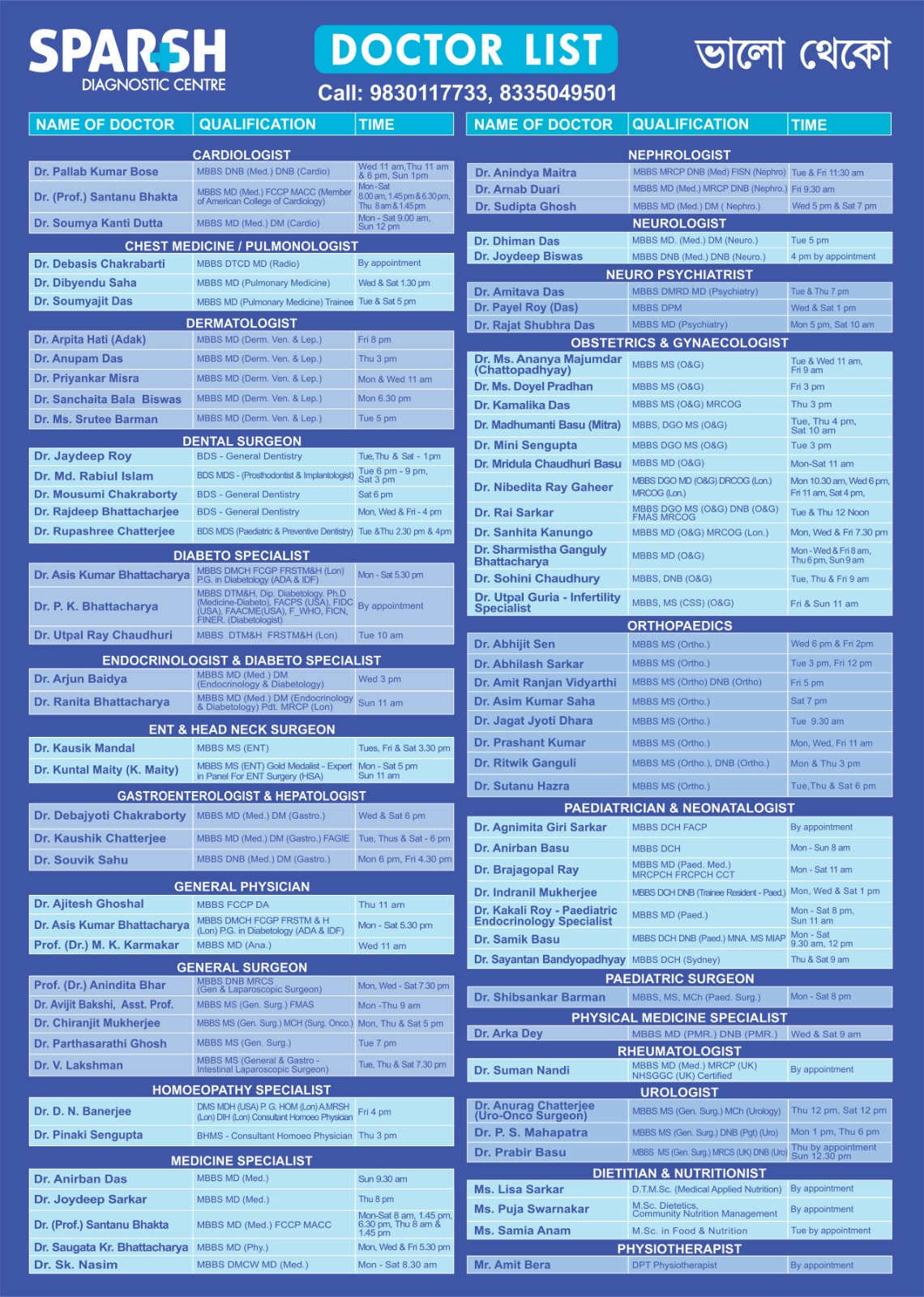
To consult a Doctor at Sparsh Diagnostic Centre, call our helpline numbers 9830117733/ 8335049501.
#BhaloTheko
Disclaimer:
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.
![]()


