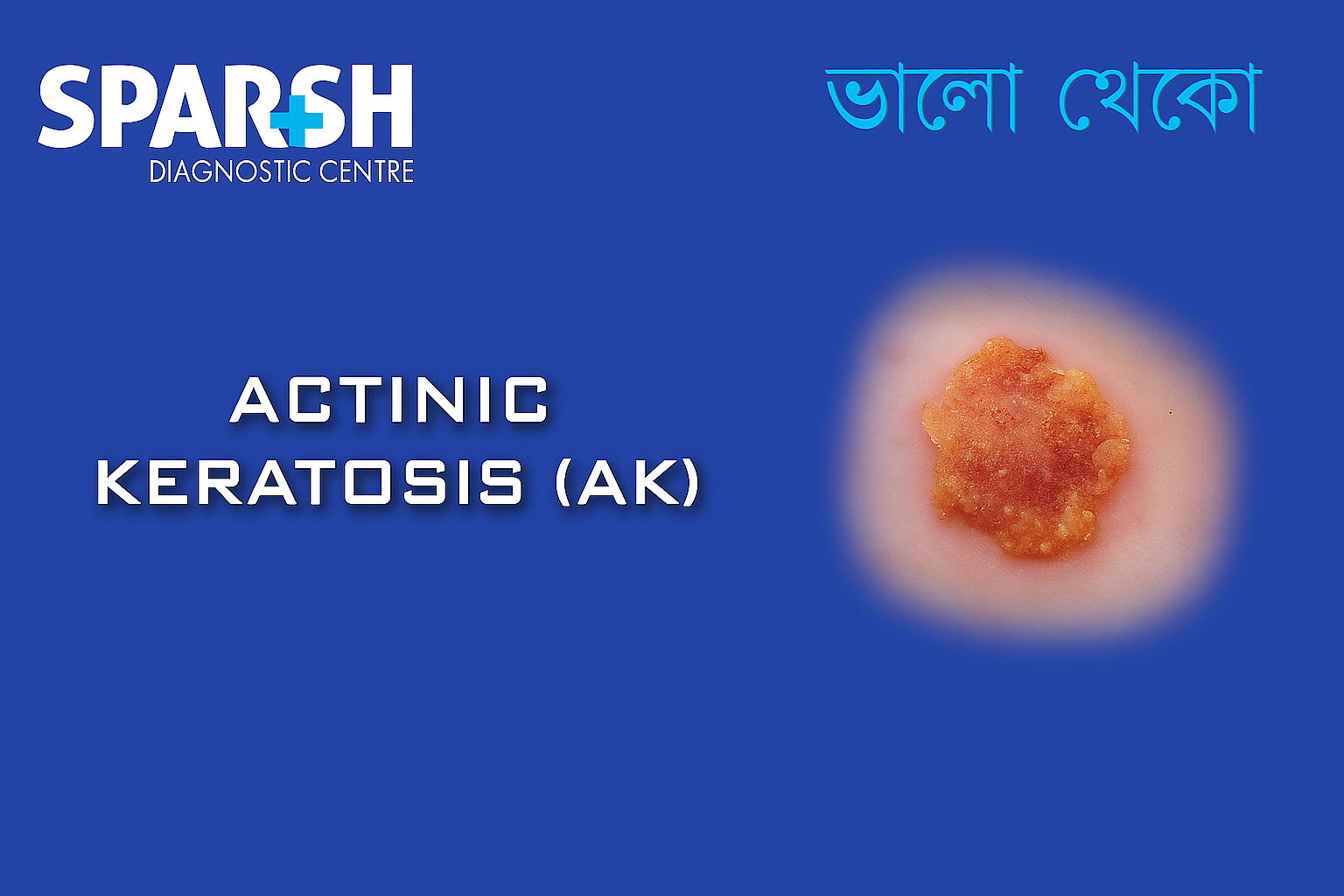
Actinic keratosis (AK), also known as solar keratosis, is a rough, scaly patch on the skin caused by excessive exposure to ultraviolet (UV) rays from the sun or artificial sources like tanning beds. While actinic keratosis itself is not cancer, it is considered a precancerous condition that can progress to squamous cell carcinoma (SCC) if left untreated.
As our understanding of skin cancer and UV damage has grown, so has awareness of actinic keratosis. Millions of people worldwide are diagnosed with AK every year, making it a significant dermatological and public health issue.
In this article, we’ll explore the causes, symptoms, risk factors, diagnostic methods, treatment options, and prevention strategies related to actinic keratosis.
What Is Actinic Keratosis?
Actinic keratosis is a common skin lesion that results from prolonged sun exposure. It usually appears on sun-exposed areas such as the:
Face
Ears
Scalp (especially in bald individuals)
Neck
Backs of the hands
Forearms
Chest
Lips (referred to as actinic cheilitis)
These lesions are often rough to the touch, with a sandpaper-like texture, and may be pink, red, brown, or skin-colored.
Although most actinic keratoses remain benign, studies show that up to 10% of lesions may evolve into squamous cell carcinoma. Hence, early identification and treatment are essential.
Causes of Actinic Keratosis
The primary cause of actinic keratosis is chronic exposure to ultraviolet (UV) radiation, especially from:
Sunlight (UVB and UVA rays)
Tanning beds or sunlamps
UV rays damage the DNA in skin cells over time. This cumulative damage leads to mutations in keratinocytes—the predominant cells in the epidermis—triggering abnormal skin growths like AK.
Risk Factors for Actinic Keratosis
Several factors can increase the likelihood of developing AK, including:
1. Excessive Sun Exposure
Spending a lot of time outdoors without sun protection significantly increases your risk.
2. Fair Skin
People with fair skin, light eyes, and blonde or red hair are more susceptible.
3. Older Age
The condition is most common in individuals over 50, due to cumulative sun exposure over time.
4. Weakened Immune System
Those undergoing immunosuppressive therapy (e.g., organ transplant recipients) are at higher risk.
5. Geographic Location
People living in sunny or high-altitude areas are more exposed to intense UV radiation.
6. History of Sunburns
Frequent or severe sunburns during childhood or adolescence can contribute to the formation of AK later in life.
Symptoms of Actinic Keratosis
Actinic keratoses can vary in appearance, but common characteristics include:
Rough, scaly, or crusty patches
Color ranging from pink, red, or brown to skin-toned
Size between 1 mm to 2 cm
Flat or slightly raised lesions
Itching, burning, or tenderness
Dry or chapped lips (in actinic cheilitis)
Sometimes, AK may be difficult to distinguish from normal skin or other lesions. That’s why it’s essential to get regular skin checks if you’re at high risk.
Types of Actinic Keratosis
There are different clinical subtypes of AK, including:
Hypertrophic AK – Thick, warty, and often scaly lesions.
Atrophic AK – Thin and less scaly, sometimes difficult to detect.
Pigmented AK – Darker in color and may resemble melanoma.
Actinic Cheilitis – Occurs on the lips, often presenting as dry and cracked lips.
Bowenoid AK – Shows features that closely mimic squamous cell carcinoma.
How Is Actinic Keratosis Diagnosed?
Diagnosis of AK is typically clinical, based on:
Physical examination
Dermoscopic evaluation
Skin biopsy (if the lesion appears suspicious or unusual)
A biopsy may be performed to rule out squamous cell carcinoma or basal cell carcinoma, especially in lesions that:
Bleed
Grow rapidly
Are ulcerated or painful
Treatment Options for Actinic Keratosis
1. Cryotherapy (Freezing)
The most common treatment
Uses liquid nitrogen to freeze the lesion
Causes the lesion to blister and fall off
2. Topical Medications
5-fluorouracil (5-FU): Destroys sun-damaged cells
Imiquimod: Stimulates the immune response
Diclofenac gel: Anti-inflammatory action
Ingenol mebutate: Works by promoting cell death
Topical therapies are ideal for treating multiple lesions or large areas of sun-damaged skin.
3. Photodynamic Therapy (PDT)
Involves applying a light-sensitive drug followed by light exposure
Targets and destroys abnormal cells
Suitable for face and scalp lesions
4. Curettage and Electrosurgery
The lesion is scraped off, and the area is cauterized
Often used for thicker or suspicious AKs
5. Laser Therapy
Ablative lasers like CO2 laser vaporize the lesion
Less commonly used due to higher costs
6. Chemical Peels
Trichloroacetic acid or other peels help in removing superficial lesions
Suitable for cosmetic improvement as well
What Happens if AK Is Left Untreated?
While many actinic keratoses may remain benign, up to 1 in 10 can progress to squamous cell carcinoma. Leaving AK untreated increases the risk of:
Cancerous transformation
Spread to other parts of the skin
Cosmetic disfigurement
Hence, early detection and management are critical.
Prevention Strategies for Actinic Keratosis
Preventing actinic keratosis primarily involves sun protection. Here are effective steps:
1. Use Sunscreen Daily
SPF 30 or higher
Broad-spectrum (UVA and UVB protection)
Reapply every 2 hours or after swimming/sweating
2. Wear Protective Clothing
Long sleeves, wide-brimmed hats, and sunglasses
3. Avoid Peak Sun Hours
Especially between 10 a.m. and 4 p.m.
4. Seek Shade
Use umbrellas or trees during outdoor activities
5. Avoid Tanning Beds
Artificial UV rays are just as harmful as natural ones
6. Regular Skin Checks
Perform monthly self-exams
Annual dermatologist visits for high-risk individuals
Living with Actinic Keratosis
Living with AK means being vigilant. Many people with actinic keratoses develop multiple lesions over time, especially if sun protection habits don’t change.
Tips for managing AK long-term:
Stick to a daily sun protection routine
Follow up with your dermatologist regularly
Treat new lesions early
Monitor for signs of SCC like rapid growth or ulceration
Early detection and consistent care can significantly reduce the risk of cancer and keep your skin healthy.
When to See a Dermatologist
You should consult a dermatologist if you notice:
New or changing skin lesions
Persistent rough patches
Lesions that bleed, itch, or hurt
A lesion that doesn’t heal
Actinic Keratosis vs Other Skin Conditions
AK can resemble several other skin issues, including:
Basal cell carcinoma or squamous cell carcinoma
A professional evaluation is essential to distinguish between these conditions accurately.
FAQs About Actinic Keratosis
Is Actinic Keratosis Curable?
Yes. AK is highly treatable when caught early. Most treatments are effective, and recurrence can be minimized with proper sun protection.
Can You Remove AK at Home?
No. Home remedies or over-the-counter treatments are not recommended. AK requires a medical diagnosis and appropriate treatment.
How Long Does Treatment Take?
Cryotherapy heals in 1–2 weeks. Topical medications may require several weeks of application.
Can AK Return After Treatment?
Yes. People with a history of AK are likely to develop new lesions. Regular follow-ups are essential.
Actinic keratosis is a warning sign from your skin—a signal that your cells have been damaged by years of sun exposure. While the condition is common and often treatable, it should never be ignored due to its potential to progress into squamous cell carcinoma.
With the right combination of sun protection, early detection, and timely treatment, actinic keratosis can be effectively managed. Regular skin exams, both self-initiated and with a dermatologist, remain your best defense in maintaining long-term skin health.
Looking for reliable skin screening and treatment options? Contact your dermatologist or visit a certified diagnostic centre today for a skin health check-up.
Let us protect your skin—because prevention is always better than cure.
#BhaloTheko
Disclaimer:
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.

![]()