
Syndrome of Inappropriate Antidiuretic Hormone secretion, commonly known as SIADH, is a disorder of water balance caused by excessive release or action of antidiuretic hormone (ADH). This condition leads to dilution of blood sodium levels, resulting in hyponatremia, which can range from mild and asymptomatic to severe and life-threatening. Early diagnosis and appropriate management are crucial to prevent serious neurological complications.
What Is Antidiuretic Hormone (ADH)?
Antidiuretic hormone, also called vasopressin, is produced in the hypothalamus and released by the posterior pituitary gland. Its primary function is to regulate water balance by controlling how much water the kidneys reabsorb.
Under normal circumstances:
ADH is released when the body is dehydrated
It helps conserve water by concentrating urine
It maintains normal blood osmolality and sodium levels
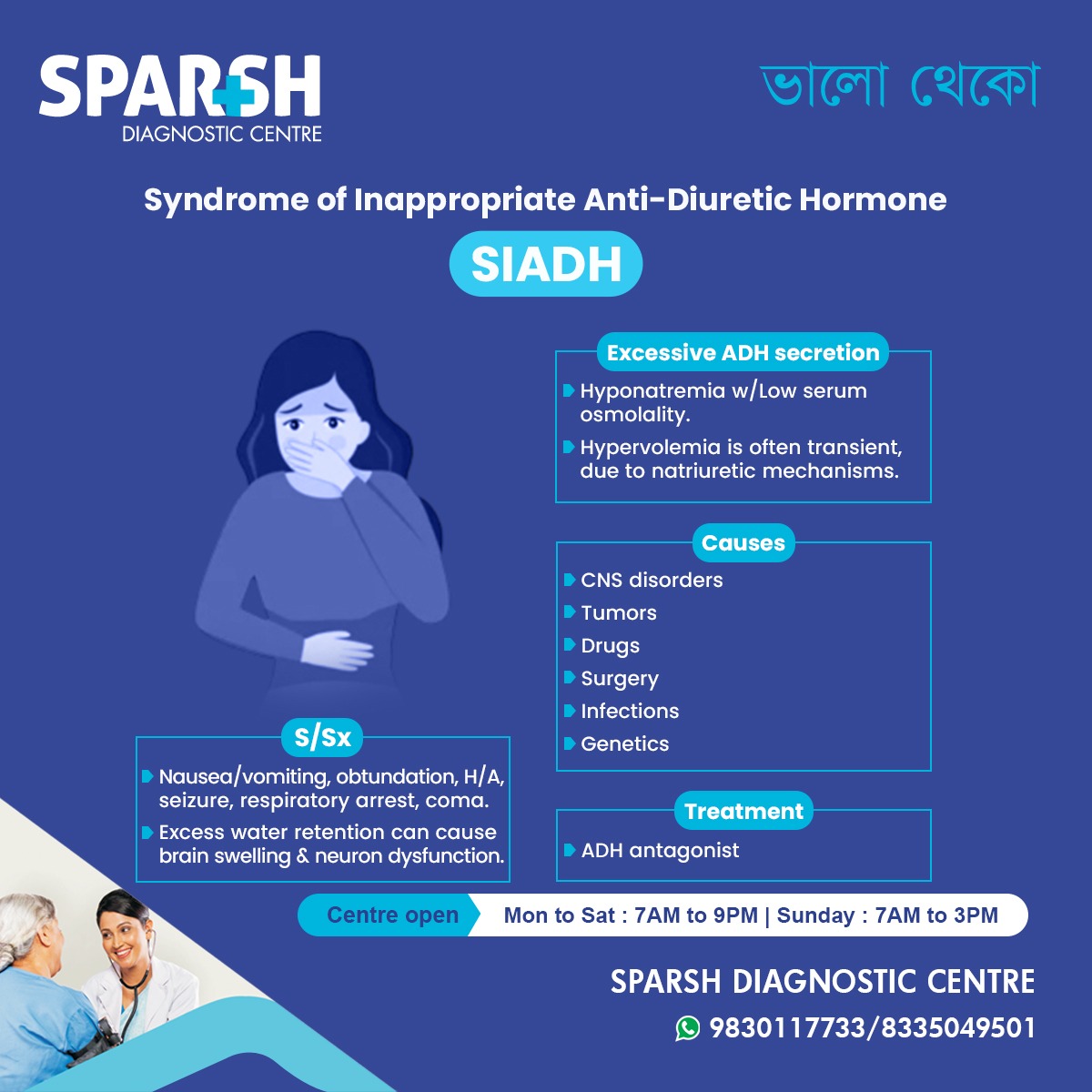
In SIADH, ADH is released inappropriately, even when the body does not need to conserve water.
What Is Syndrome of Inappropriate Antidiuretic Hormone (SIADH)?
SIADH is a condition characterized by:
Excessive ADH secretion
Increased water retention
Dilutional hyponatremia
Low serum osmolality
Inappropriately concentrated urine
Despite excess water retention, patients often appear euvolemic, meaning they do not show obvious signs of fluid overload like edema.
Pathophysiology of Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
The underlying mechanism of SIADH involves:
Persistent ADH action on the kidneys
Increased water reabsorption in the collecting ducts
Dilution of sodium in the blood
Suppression of aldosterone and increased natriuresis (sodium loss in urine)
This combination leads to low sodium levels without significant fluid accumulation in tissues.
Causes of Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
SIADH can be triggered by a wide range of medical conditions and external factors.
1. Central Nervous System Disorders
Head injury
2. Malignancies
Certain tumors can produce ADH ectopically.
3. Pulmonary Conditions
Mechanical ventilation
4. Medications
Antidepressants (SSRIs, TCAs)
Antipsychotics
Antiepileptics (carbamazepine)
5. Post-operative States
Major surgery
Pain and stress response
Anesthesia-related ADH release
6. Infections
7. Genetic and Idiopathic Causes
In some patients, no clear cause is identified.
Risk Factors for Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Individuals at higher risk include:
Elderly patients
Cancer patients
Patients on long-term psychotropic medications
Those with recent brain or lung disease
Hospitalized or critically ill patients
Signs and symptoms of Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Symptoms depend largely on:
Severity of hyponatremia
Speed of sodium decline
Mild Symptoms
Moderate Symptoms
Confusion
Muscle cramps
Weakness
Restlessness
Severe Symptoms
Vomiting
Decreased consciousness
Coma
Rapid onset hyponatremia is particularly dangerous due to cerebral edema.
Complications of Untreated Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
If not treated promptly, SIADH can lead to:
Brain swelling
Permanent neurological damage
Seizures
Respiratory failure
Death
Overcorrection of sodium can also cause osmotic demyelination syndrome, a serious neurological condition.
Diagnosis of Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Diagnosing SIADH involves a combination of clinical evaluation and laboratory testing.
Key Diagnostic Criteria
Serum sodium <135 mmol/L
Low plasma osmolality
Inappropriately high urine osmolality
Elevated urine sodium
Normal renal, adrenal, and thyroid function
Clinical euvolemia
Additional Tests
Chest imaging
Brain imaging if CNS cause suspected
Early and accurate diagnosis is essential for safe management.
Differential Diagnosis
Conditions that may mimic SIADH include:
These must be ruled out before confirming SIADH.
Management and Treatment of Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
Treatment depends on:
Severity of symptoms
Sodium levels
Underlying cause
1. Fluid Restriction
First-line therapy in most cases
Typically 800–1000 mL/day
2. Treat Underlying Cause
Stop offending medications
Treat infections or tumors
Manage CNS or pulmonary disease
3. Hypertonic Saline
Used in severe or symptomatic hyponatremia
Administered carefully under monitoring
4. ADH Antagonists (Vaptans)
Block ADH receptors
Increase free water excretion
Used in resistant cases
5. Oral Salt or Urea
Helps increase serum sodium in chronic cases
Monitoring During Treatment
Careful monitoring is critical to prevent complications:
Frequent sodium level checks
Strict fluid balance monitoring
Neurological assessment
Sodium correction should not exceed 8–10 mmol/L per 24 hours.
Prognosis of Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
The outcome depends on:
Speed of diagnosis
Severity of hyponatremia
Underlying cause
With appropriate treatment:
Most patients recover well
Chronic cases require long-term monitoring
Prognosis is poorer when associated with malignancy
Prevention and Patient Awareness
While SIADH cannot always be prevented, risk can be reduced by:
Regular monitoring in high-risk patients
Medication review
Early evaluation of neurological or respiratory symptoms
Prompt laboratory testing for unexplained symptoms
Frequently Asked Questions (FAQs)
What is the most common cause of SIADH?
Malignancy, particularly small cell lung cancer, is one of the most common causes.
Is SIADH a life-threatening condition?
Yes, severe or rapidly developing hyponatremia can be life-threatening if untreated.
Can SIADH be cured?
SIADH is often reversible if the underlying cause is treated successfully.
What sodium level is dangerous in SIADH?
Levels below 120 mmol/L are considered severe and require urgent medical care.
How is SIADH different from dehydration?
SIADH involves excess water retention, while dehydration involves fluid loss.
Can SIADH recur?
Yes, especially if the underlying cause persists or recurs.
Is fluid restriction always required?
In most cases, yes, but treatment is individualized.
Which tests confirm SIADH?
Blood sodium, serum osmolality, urine osmolality, and urine sodium tests.
Syndrome of Inappropriate Antidiuretic Hormone is a complex but treatable condition that requires timely recognition and careful management. Understanding its causes, symptoms, and diagnostic criteria helps prevent serious complications. With modern diagnostic tools and targeted therapies, patients with SIADH can achieve excellent outcomes when treated promptly and appropriately.
#BhaloTheko
Disclaimer:
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.
Sparsh Doctor List
![]()


