Hyperchloremia is a metabolic condition that often goes unnoticed until detected through routine blood tests. Although it may sound uncommon, elevated chloride levels in the blood can significantly affect the body’s acid–base balance and overall health. Understanding hyperchloremia is important, especially for individuals with kidney disorders, dehydration, or chronic illnesses.
This article explains what hyperchloremia is, why it occurs, how it affects the body, and what can be done to manage it effectively.
What Is Hyperchloremia?
Hyperchloremia is a condition characterized by abnormally high levels of chloride in the blood. Chloride is an essential electrolyte that helps maintain fluid balance, regulate blood pressure, and support proper nerve and muscle function.
In healthy adults, normal blood chloride levels typically range between 96 and 106 mEq/L. When chloride levels rise above this range, hyperchloremia may develop.
Chloride works closely with sodium, potassium, and bicarbonate to maintain the body’s acid–base balance (pH). When chloride levels become excessively high, this balance is disrupted, often leading to metabolic acidosis, a condition in which the blood becomes too acidic.

Why is Chloride Important in the Body
Chloride plays several vital roles, including:
Maintaining proper hydration by balancing fluids inside and outside cells
Helping regulate blood pressure
Supporting digestion by forming hydrochloric acid in the stomach
Assisting in nerve signal transmission
Helping maintain acid–base equilibrium
Because chloride is so closely tied to fluid and electrolyte balance, changes in its concentration often reflect broader systemic issues.
Causes of Hyperchloremia
Hyperchloremia usually develops as a result of fluid loss, kidney dysfunction, or medical treatments that alter electrolyte levels. Common causes include:
1. Dehydration
Severe dehydration due to vomiting, diarrhea, excessive sweating, or inadequate fluid intake can concentrate chloride levels in the blood.
2. Excessive Saline Infusion
Receiving large volumes of normal saline (0.9% sodium chloride) during intravenous fluid therapy can increase chloride levels, especially in hospitalized patients.
3. Kidney Disorders
The kidneys regulate electrolyte balance. Conditions such as:
can impair chloride excretion, leading to accumulation.
4. Gastrointestinal Loss of Bicarbonate
Prolonged diarrhea or intestinal fistulas can cause loss of bicarbonate, which raises chloride levels to maintain electrical neutrality.
5. Certain Medications
Some drugs can contribute to hyperchloremia, including:
Diuretics
Carbonic anhydrase inhibitors
Ammonium chloride
6. Endocrine and Metabolic Conditions
Conditions such as diabetes, adrenal disorders, or severe infections can disrupt electrolyte regulation and lead to elevated chloride.
Symptoms of Hyperchloremia
Mild hyperchloremia may not cause noticeable symptoms and is often detected incidentally through blood tests. However, moderate to severe cases can produce a range of symptoms.
Common Symptoms Include:
Dry mouth and dehydration
Breathing difficulties
Rapid or deep breathing (Kussmaul breathing)
Confusion or reduced cognitive function
Severe Symptoms May Include:
Fever and sweating
Worsening kidney function
Symptoms often overlap with those of the underlying condition causing hyperchloremia, making proper diagnosis essential.
Hyperchloremia and Metabolic Acidosis
One of the most important clinical associations of hyperchloremia is hyperchloremic metabolic acidosis.
In this condition:
Bicarbonate levels decrease
Chloride levels increase
Blood pH drops
This type of acidosis is commonly seen in:
Chronic diarrhea
Renal tubular acidosis
Excessive saline administration
Metabolic acidosis can impair enzyme function, reduce cardiac output, and increase the workload on the lungs.
Who Is at Higher Risk?
Certain groups are more prone to developing hyperchloremia:
Patients with chronic kidney disease
Individuals with prolonged diarrhea or vomiting
Hospitalized patients receiving IV fluids
People with uncontrolled diabetes
Elderly individuals with reduced kidney function
Critically ill patients in intensive care units
Diagnosis of Hyperchloremia
Hyperchloremia is diagnosed through blood tests, most commonly as part of an electrolyte panel or comprehensive metabolic panel.
Diagnostic Tests May Include:
Serum chloride test
Serum sodium and potassium levels
Bicarbonate levels
Blood urea nitrogen (BUN) and creatinine
Arterial blood gas (ABG) analysis (if acidosis is suspected)
Doctors interpret chloride levels in conjunction with other electrolytes to identify the underlying cause rather than relying on chloride levels alone.
Treatment of Hyperchloremia
Treatment focuses on addressing the underlying cause rather than simply lowering chloride levels.
Common Treatment Approaches:
1. Fluid Replacement
Oral rehydration or IV fluids adjusted to avoid excess chloride
Balanced solutions may be preferred over normal saline
2. Correcting Acid–Base Imbalance
Bicarbonate therapy may be used in severe metabolic acidosis
Monitoring blood pH and electrolyte levels is essential
3. Treating Underlying Conditions
Managing kidney disease
Controlling diarrhea or vomiting
Adjusting medications that affect electrolyte balance
4. Dietary Modifications
Adequate hydration
Reduced intake of high-salt processed foods if advised by a healthcare provider
Treatment plans are individualized based on severity, symptoms, and overall health status.
Can Hyperchloremia Be Prevented?
While not all cases are preventable, certain measures can reduce risk:
Maintain proper hydration
Avoid excessive use of saline without medical supervision
Manage chronic illnesses effectively
Follow prescribed medication instructions carefully
Undergo regular blood tests if you have kidney disease or metabolic disorders
When to See a Doctor
Medical attention should be sought if symptoms such as persistent thirst, confusion, breathing difficulties, or severe fatigue occur—especially in individuals with known kidney or metabolic conditions.
Early detection through routine diagnostic testing can prevent complications and improve outcomes.
Frequently Asked Questions (FAQs)
1. Is hyperchloremia dangerous?
Mild hyperchloremia may not be dangerous, but severe or untreated cases can lead to metabolic acidosis, kidney strain, and cardiovascular complications.
2. Can hyperchloremia go away on its own?
In cases caused by temporary dehydration or fluid imbalance, chloride levels may normalize with proper hydration. Chronic cases require medical treatment.
3. What foods increase chloride levels?
Chloride is commonly consumed as sodium chloride (salt). Excessive intake of processed and salty foods may contribute, especially in people with kidney issues.
4. Is hyperchloremia the same as high sodium?
No. Although chloride often rises alongside sodium, they are separate electrolytes. Hyperchloremia can occur even when sodium levels are normal.
5. How is hyperchloremia different from hyponatremia?
Hyperchloremia refers to high chloride levels, while hyponatremia refers to low sodium levels. Both involve electrolyte imbalance but have different causes and treatments.
6. Can children develop hyperchloremia?
Yes, particularly in cases of severe dehydration, diarrhea, or certain metabolic disorders.
7. How long does treatment take?
Recovery depends on the underlying cause. Some cases resolve within days, while others require long-term management.
Key Takeaway
Hyperchloremia is more than just a lab abnormality—it reflects an underlying imbalance that can affect vital bodily functions. While often mild and manageable, it should not be ignored, especially in individuals with kidney disease, dehydration, or chronic illness. Early diagnosis, proper treatment, and regular monitoring are crucial for maintaining electrolyte balance and overall health.
#BhaloTheko
Disclaimer:
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.
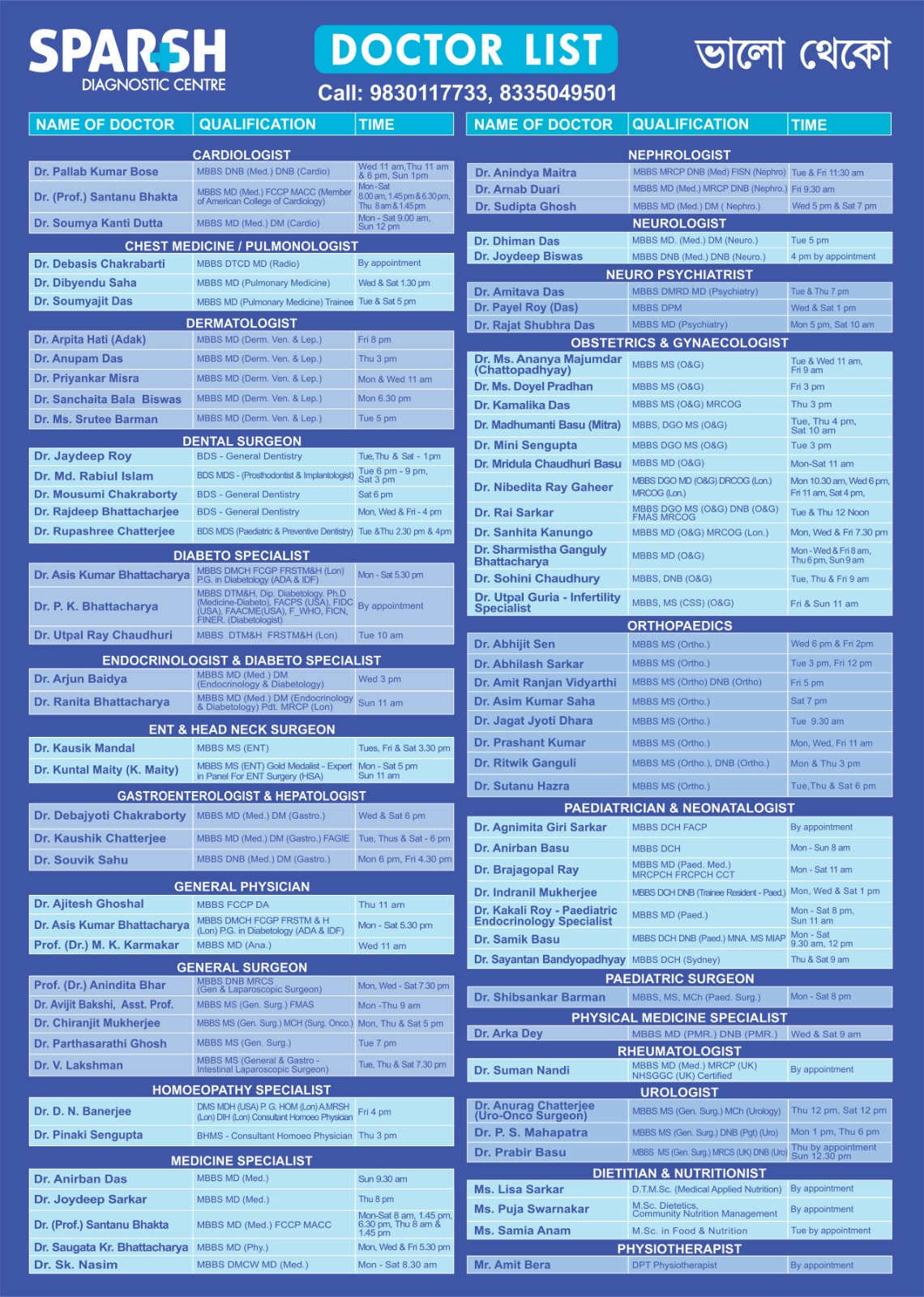
Sparsh Doctor List
![]()